Treating a pelvic ischial tuberosity fracture
A 16-year-old male track and cross-country athlete presented with pain high up in his right posterior thigh. He had sustained an injury two weeks prior while sprinting during a track event, feeling a sharp pain below his right buttock, which caused him to collapse to the ground in pain.
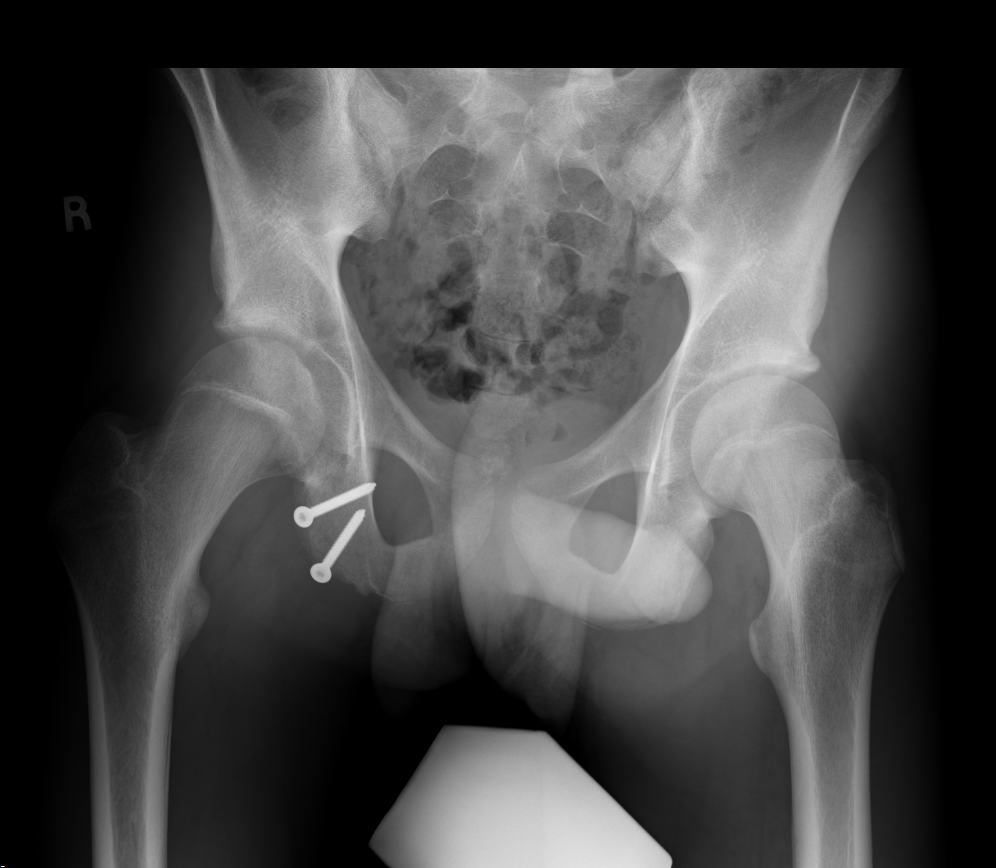
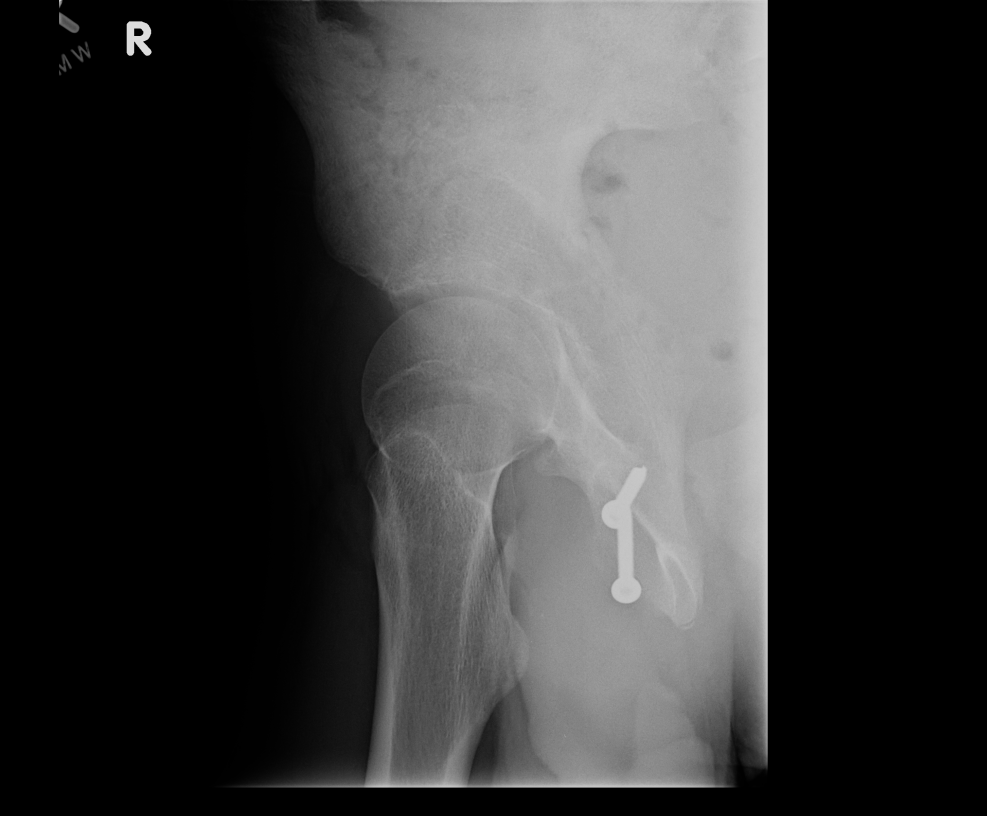
The patient had x-rays done at an outside office, which showed that he had suffered a pelvic ischial tuberosity avulsion fracture. He was referred to Boston Children’s, where he was seen by primary care sports medicine physician Michael O’Brien, MD. Due to the degree of displacement with this fracture, operative treatment was discussed as a potential option, and the patient was referred to Benton Heyworth, MD, a pediatric orthopedic surgeon in Boston Children’s Orthopedics and Sports Medicine Center.
In the majority of pelvic ischial tuberosity fractures, the bone fragment is displaced from the pelvis by less than 1 or 2 cm. But in this patient’s case, the bone was 4 cm displaced. With the displacement being so severe, there was cause for concern regarding the functional outcome following non-operative treatment. Such injuries that fail to heal after non-operative treatment can result in a non-union or generate heterotopic

Operative treatment of these fractures can be somewhat invasive, compared to other fractures in adolescent athletes. The surgery is an involved and complex procedure that requires an initial incision greater than 8 cm. Furthermore, the area of the fracture is deep within the back of the thigh and pelvis region, requiring the gluteus muscle be elevated out of the way and careful inter-operative dissection and protection of the sciatic nerve. The hardware used in this procedure — generally two to three screws — can be a source of discomfort for the patient, and may require a secondary surgery to remove the screws.
The relative risks and benefits of surgical versus nonsurgical treatment were discussed with the patient and his family. As an elite track athlete with collegiate athletic aspirations, the patient was concerned about any compromise to his highest level of function. At the conclusion of this shared decision-making process, the patient decided to proceed with surgery.
Inter-operatively, two screws were used to reattach the bone fragment to the pelvis. Following complete healing, the patient has experienced no discomfort from the hardware, and a secondary surgery has not been needed to date. 4-5 months out from surgery, the patient was back to running competitively and has no pain, discomfort or perceived weakness during competition.