What is clubfoot?
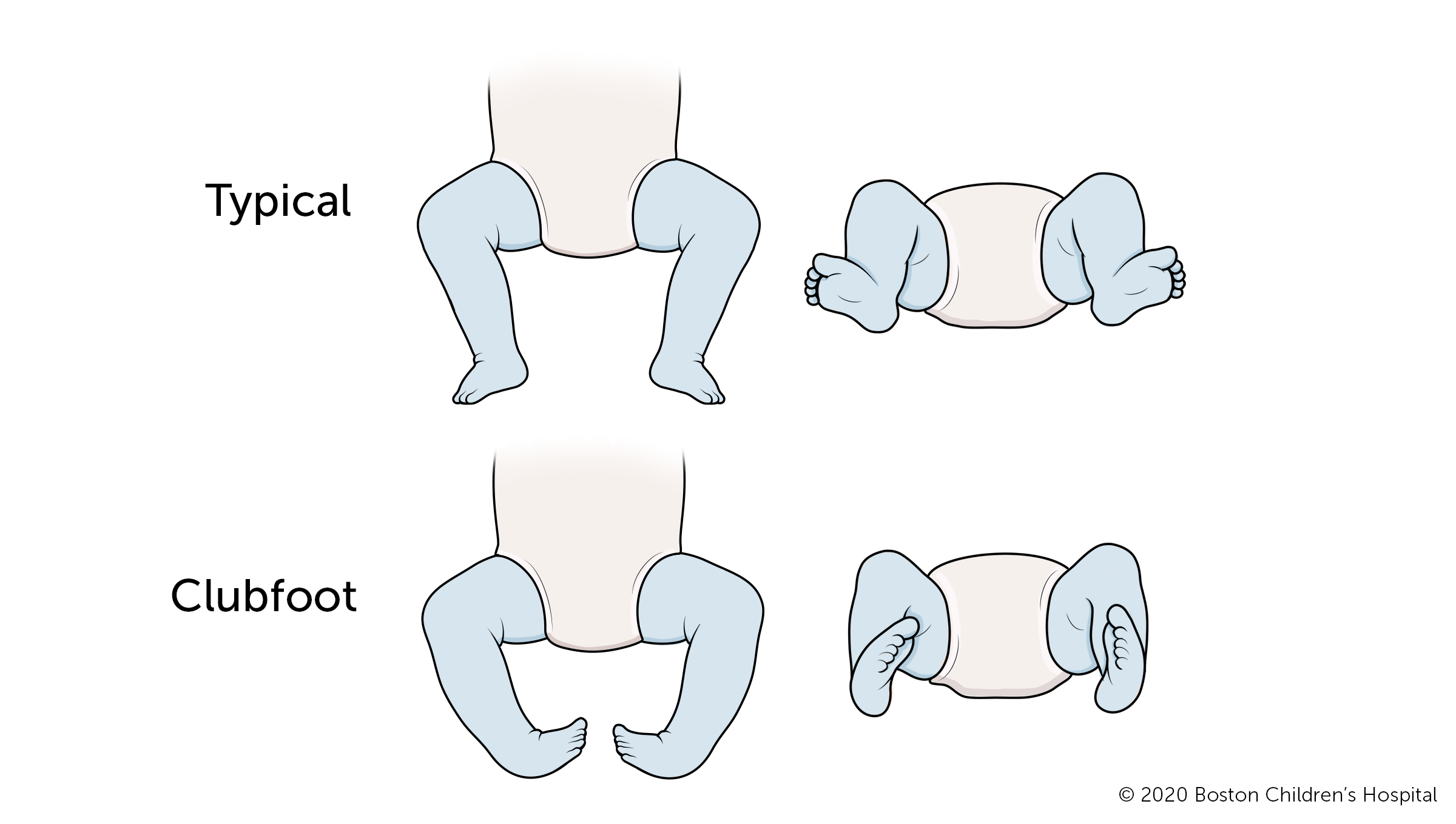
Clubfoot is a congenital foot deformity that affects a child’s bones, muscles, tendons, and blood vessels. The front half of an affected foot turns inward and the heel points down. In severe cases, the foot is turned so far that the bottom faces sideways or up rather than down. The condition, also known as talipes equinovarus, is fairly common. About one to four of every 1,000 babies are born with clubfoot. The condition affects boys twice as often as it does girls.
About 50 percent of children with clubfoot have it in both feet, a condition known as bilateral clubfoot. Many parents find out their child has clubfoot during a prenatal ultrasound months or weeks before their child is born. Once the child is born, the condition is clearly visible. Ideally, treatment begins in the first month of a child’s life.
Despite the appearance, clubfoot is not a painful condition for babies. Almost all children who receive early treatment are able to run, play, and function quite normally. Without treatment, clubfeet do not get better on their own. The foot remains in the deformed position and makes it hard for a child to walk.
What are the symptoms of clubfoot?
Clubfoot is readily visible when a baby is born.
- The front half of the foot turns inward and the heel points downward.
If only one foot is affected:
- The calf muscle on the affected leg is smaller than on the other leg.
- The leg on the affected side is often shorter than on the other side.
- The affected foot may be short and wide.
Who’s at risk for developing clubfoot?
Most children with clubfoot do not have a parent with the condition. However, having an older sibling with clubfoot increases a baby’s risk of being born with the condition.
- If a boy has a clubfoot, there’s a 2.5 percent chance that his next-born sibling will have clubfoot, too.
- If a girl has a clubfoot, there’s a 6.5 percent chance that her next-born sibling will be born with clubfoot.
Other risk factors include:
- male gender; boys are born with clubfoot twice as often as girls
- genetic syndromes, such as Edwards syndrome (trisomy 18)
- neuromuscular disorders, such as cerebral palsy (CP) and spina bifida
- birth defects, such as arthrogryposis and amniotic band syndrome
- oligohydramnios, a decreased amount of amniotic fluid surrounding the fetus in the uterus during pregnancy
- breech birth, being born bottom first rather than head first
Babies born with clubfoot may also be at increased risk of having an associated hip condition, hip dysplasia. In hip dysplasia, the top of the thigh bone (femur) slips in and out of its socket, because the socket is too shallow to keep the joint intact.

Meet Finn
When Finn's parents have to chase him around the house to put on his clubfoot brace, they consider it a win. "Parents should know that clubfoot is completely treatable," says his mom.
What causes clubfoot?
Most clubfeet are “idiopathic,” meaning that doctors don’t know for sure what causes them. Clubfoot probably has a genetic component and runs in families. But researchers don’t yet know what gene (or set of genes) is responsible.
In all children with clubfeet, tightness of the muscles and tendons around the foot and ankle keep the foot in the characteristic downward and inward position. This tightness may be related to differences in blood circulation or how nerves receive signals in the affected legs. Other theories for the causes of clubfeet include defects in development of the bones, tendons, or muscles or some mechanical obstruction in utero. However, these theories have not yet been proven.
In some cases, clubfoot is part of a syndrome or birth defect. In other cases, the foot was in an awkward position in the mother’s womb. But most of the time, children are born with clubfoot for no known reason.
What are the different types of clubfoot?
There are two types of clubfoot, each with different causes.
Idiopathic clubfoot
The most common type of clubfoot is idiopathic, which means the cause is unknown. Idiopathic clubfoot is not related to any other medical problems. Feet of babies with this type of clubfoot are stiff and hard to manipulate.
Syndromic clubfoot
Syndromic clubfoot occurs when the condition is part of a larger syndrome. This type is usually more severe and difficult to treat.
Clubfoot | Diagnosis & Treatments
How is clubfoot diagnosed?
Most of the time, a baby’s clubfoot is diagnosed during a prenatal ultrasound before they are born. About 10 percent of clubfeet can be diagnosed as early as 13 weeks into pregnancy. By 24 weeks, about 80 percent of clubfeet can be diagnosed, and this number steadily increases until birth.
If a child is not diagnosed before birth, clubfoot can be seen and diagnosed as soon as they are born. A physical exam is generally all that is necessary to establish a diagnosis. In rare cases other tests may be used, including:
- x-ray
- computerized tomography scan (CT or CAT scan)

When your baby has clubfoot: Advice for expecting parents
“Our goal when we meet with parents is to reassure them that clubfoot is treatable.”
How is clubfoot treated?
The goal of clubfoot treatment is to correct the position of the foot so that the bones, tendons, and muscles of the foot can grow more normally. Ideally, treatment begins within one month of a child’s birth, when their feet and ankles are at the earliest possible stage of development.
Ponseti method
The Ponseti method is the most common and effective clubfoot treatment. This treatment uses a series of casts and braces to rotate the baby’s foot into a corrected position. The foot is rotated externally until it is turned out 60-70 degrees. Treatment usually begins sometime between birth and 4 weeks of age and involves two stages: treatment and bracing.
Treatment stage
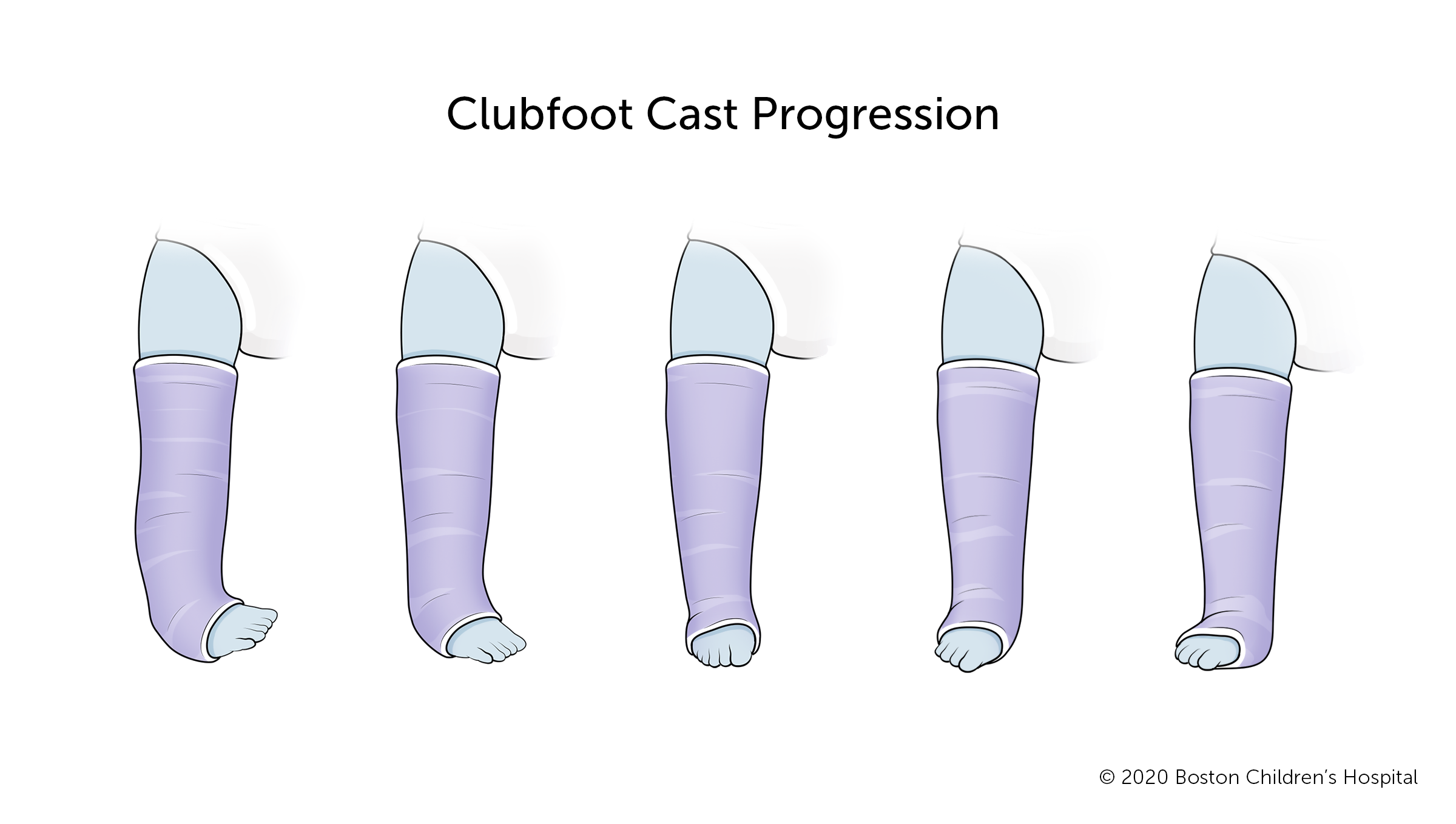
During the treatment stage, your child’s doctor will slowly reposition your child’s foot using a series of casts. This stage involves two to three months of stretching and repositioning the foot.
- The doctor will stretch and reposition your child’s foot, then place their foot, ankle, and leg in a cast to hold the foot in the new position.
- The cast will be removed after about a week, and the doctor will once again reposition your child’s foot. A new cast will hold the foot in its new position.
- This process will be repeated every week until your child’s foot is moved from its incorrect inward-facing position to the correct outward position. Typically, it takes five to eight readjustments and cast changes to move the foot into a correct position.
- When the foot is in its improved outward position, most children need minor surgery (tenotomy) to lengthen their Achilles tendon. This is the cord that attaches the calf muscle to the heel. About 95 percent of babies need this surgery, which is usually performed under local anesthesia.
See tips for cast care and maintenance.
Clubfoot bracing stage
Clubfoot bracing lasts for several years and is crucially important to your child’s long-term mobility. The brace maintains your child’s foot in a corrected position.
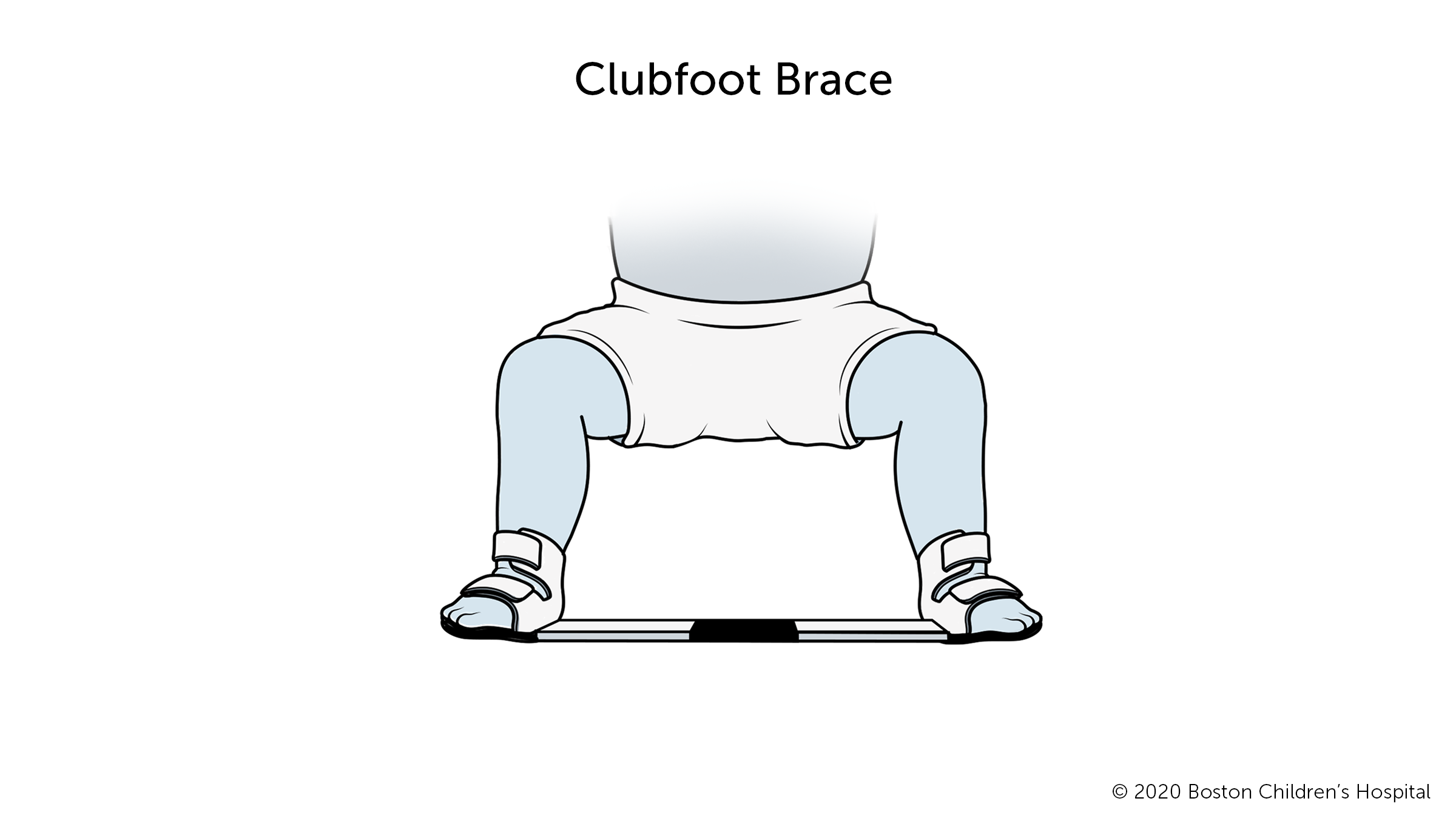
- From the end of the treatment stage until your child is 3 to 6 months old, they will wear the brace about 22 hours a day.
- After this initial period, your child’s doctor will probably say it’s OK for your child to wear the brace at night and at nap time, about 15 or 16 hours a day.
- When your baby is ready to learn how to crawl, and then walk, run, and play, they can do so with the brace off.
- You will need to follow the bracing program strictly until your child is 4 years old. Despite the inconvenience, this is the best way to prevent your child’s foot from turning inward again and needing further medical intervention.
What is the long-term outlook for babies with clubfoot?
With early treatment and bracing, almost all babies with clubfoot grow up to have normally functioning feet. They can run, play, and wear normal shoes. If only one foot is affected, it will most likely be smaller and somewhat less mobile than the other foot. Your child may require two different shoe sizes. The affected leg may be slightly smaller and the calf may be less muscular than their other leg.
While clubfoot responds well to treatment, it does not get better on its own. If left untreated, clubfoot will become worse with age and make it hard for your child to walk. Therefore, early treatment and following the bracing program closely are very important.
How we care for clubfoot at Boston Children’s Hospital
The Lower Extremity Program at Boston Children's Hospital takes a conservative, non-surgical approach to clubfoot whenever possible, and we have excellent success rates. In the rare case that a newborn needs surgery, we work with the Department of Anesthesiology, Critical Care and Pain Medicine to avoid the use of general anesthesia whenever we can.
We offer an especially strong and supportive bracing program. We also work with the Fetal Care and Surgery Center, the hospital’s prenatal counseling program, to help parents anticipate and plan for their baby’s care after birth.

