What are spondylolysis and spondylolisthesis?
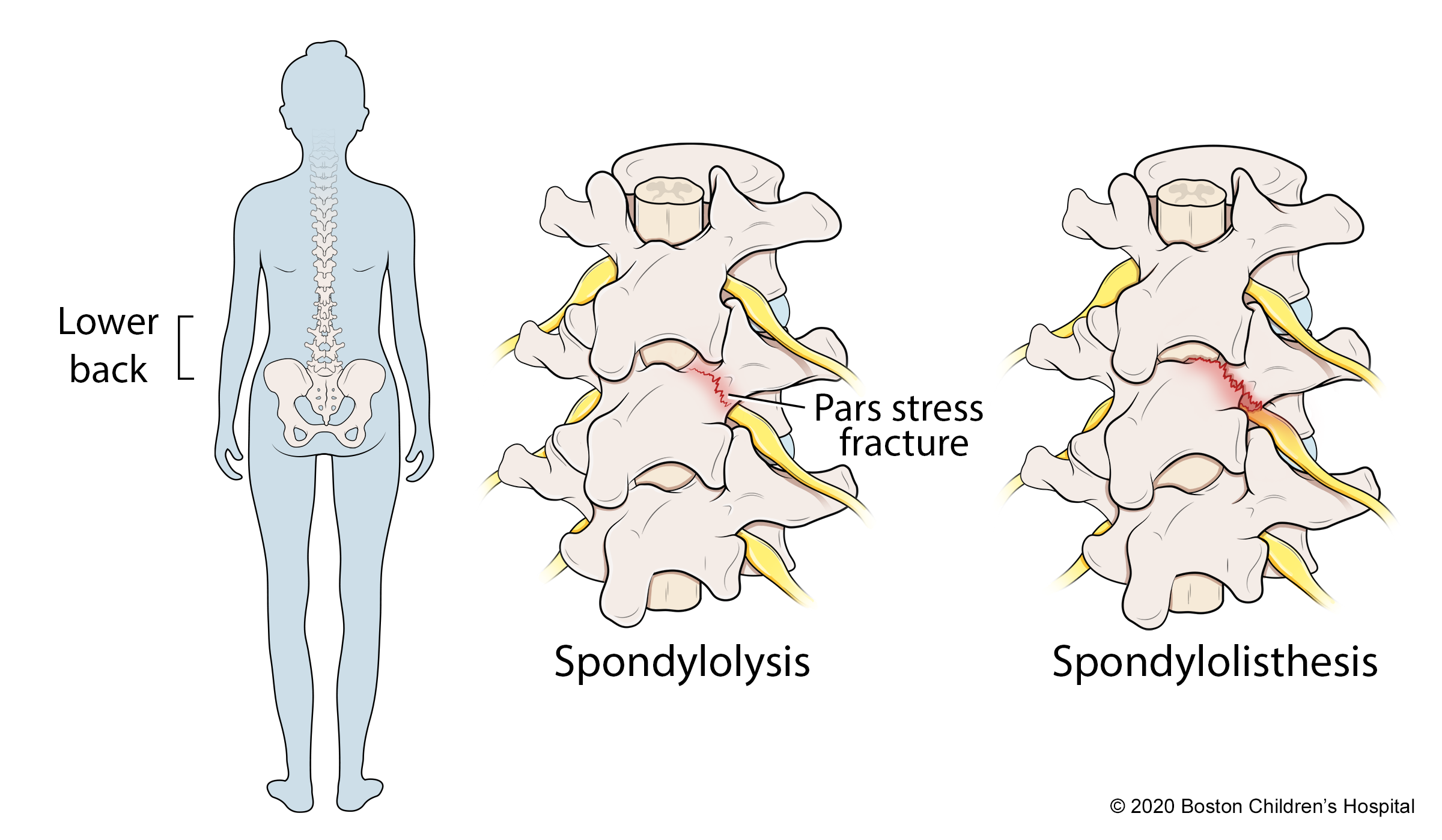
Spondylolysis is a stress fracture in the lower back. Children and teens who participate in sports that put repetitive stress on the low back, such as gymnastics, skiing, and weightlifting, are at highest risk. Some children are born with a genetic tendency to develop spondylolysis even if they do not participate in sports.
If left untreated, spondylolysis can progress to spondylolisthesis, a condition in which a vertebra, weakened by fracture, slips out of alignment with the rest of the spine. The risk of spondylolysis is higher during growth spurts.
Athletes with either condition can usually return to sports after several months of rest and physical therapy. Your child may need to wear a back brace as part of their recovery. If a vertebra is severely out of alignment, or if your child remains in pain despite other forms of treatment, they may need spinal fusion surgery, although the need for this is rare.
Anatomy of the spine
The spine has 24 vertebrae, small, rectangular bones stacked on top of each other along the length of the back. Soft intervertebral disks sit between each vertebra and provide cushioning. There is a section of the vertebra called the pars interarticularis that connects the facet joints at the back of the spine. This structure of the spine allows it to bend and twist while also stabilizing the back and protecting the spinal cord.
The pars interarticularis is vulnerable to fracture, particularly with repetitive extensions, in other words, repeatedly bending backwards as in gymnastics, for instance. With spondylolysis, the fracture may occur on one or both sides of the bone. A vertebra with stress fractures on both sides is more likely to slip out of alignment, leading to spondylolisthesis.
What causes spondylolysis and spondylolisthesis?
Repetitive stress
Most cases of spondylolysis and spondylolisthesis are repetitive stress injuries that develop during intense athletic training. Athletes who participate in sports that put repeated pressure on the lower back, such as gymnastics, rowing, diving, downhill ski racing, and weightlifting, are particularly prone to these overuse injuries of the spine. As the athlete’s muscles become overly fatigued, the load is transferred to their bones. Over time, the continued pressure can cause stress fractures in the lumbar spine.
Genetic causes
Some children are born with fragile spines that can fracture in the course of normal childhood activities. These children may have lower spine fractures by the age of 5 or 6, usually with no signs or symptoms. Typically, they are diagnosed only if their doctor orders an x-ray for another back issue.
What are the symptoms of spondylolysis and spondylolisthesis?
Spondylolysis is one of the most common causes of low back pain in young athletes. The degree of pain depends, in part, on the severity of the injury. For those with spondylolisthesis, the further a vertebra slips out of alignment, the greater the pain the child may experience (and the more likely they are to need surgery).
Symptoms of spondylolysis include:
- low back pain that increases during physical activity
- pain that spreads to the buttocks and down the back of the thighs
- tight hamstrings
In addition to low back pain, other symptoms of spondylolisthesis include:
- muscle spasms in the back of the thighs (hamstrings)
- tight hamstrings that may force the child to walk in shorter strides
- numbness or tingling sensations in the foot
Back pain caused by spondylolysis or spondylolisthesis tends to progress in stages, starting out mild and gradually becoming more persistent. In severe cases, the pain can become constant, even when the child is not active.
It’s important to note that low back pain is often a symptom of muscle strain, not a fracture. Either way, if your child has low back pain, they should be seen by a spine or sports medicine specialist. Prompt treatment can help resolve the pain and prevent the injury from progressing.
How we care for spondylolysis at Boston Children’s Hospital
The Spine and Sports Program at Boston Children’s Hospital focuses on spine conditions and injuries that affect young athletes. Our team includes sports medicine physicians, physical therapists, and athletic trainers who work with young athletes with a focus on recovery and safe return to play.
As part of the Orthopedic and Sports Medicine Center, we have access to an extensive network of specialists and resources that enables us to tailor treatment to each individual’s situation and needs. We collaborate regularly with colleagues throughout the hospital and The Micheli Center for Sports Injury Prevention to provide an accurate diagnosis and prompt, effective treatment for each of our patients.
Spondylolysis and Spondylolisthesis | Diagnosis & Treatments
How are spondylolysis and spondylolisthesis diagnosed?
The first step in diagnosing spondylolysis or spondylolisthesis is a physical exam. Your child’s doctor may order x-rays to look for a fracture. But because some stress fractures do not show up on x-rays, your child’s doctor may also order one or more of the following tests:
Computerized tomography scan (also called a CT or CAT scan) is an imaging procedure that uses a combination of x-rays and computer technology to produce cross-sectional images of the spine. CT scans are more detailed than general x-rays.
A bone scan is an imaging technique that uses a special dye that circulates through the bloodstream to help clinicians visualize bone metabolism and cell activity. If a stress fracture appears “hot” on the scan, it suggests that the injury has happened recently.
Magnetic resonance imaging (MRI) is an imaging procedure that uses a combination of large magnets, radiofrequencies, and a computer to produce detailed images of the organs and structures of the body. MRIs are particularly helpful to determine if a fracture is old or new.
What are the treatment options for spondylolysis and spondylolisthesis?
Non-surgical treatment
The primary treatment for spondylolysis and mild-to-moderate spondylolisthesis is time off from sports and other activities. This gives your child’s spine time to heal.
In addition to rest, your child's doctor may recommend physical therapy and bracing.
- Physical therapy focuses on stretching the hamstrings in the backs of the legs, strengthening the core muscles that support the spine, and increasing mobility.
- Bracing works by holding the spine in an upright position. If your child is in a lot of pain when they lean backward, they may need to wear a back brace for as long as four months.
- In some cases, doctors recommend bone growth stimulation. A bone growth stimulator is a device that delivers weak electrical currents to the area around a fracture that has not healed. This can promote the growth of new bone. The device may be worn next to the skin or implanted under the skin.
Surgical treatment
Spinal fusion surgery is usually only recommended for children with severe spondylolisthesis whose vertebra has slipped far out of alignment, or when the slippage continues to progress despite other treatments. In rare cases, surgery is the best option for children with spondylolysis if they are still in pain after non-surgical treatment.
During spinal fusion surgery, a surgeon realigns the vertebrae and places small chips of bone (bone graft) around the injured area. They may also stabilize the spine with metal rods and screws to hold the vertebrae in place as the bones fuse. Over time, this section of the spine will become solid bone in a process similar to the way other bones in the body heal if they are broken.
What is the long-term outlook for spondylolysis and spondylolisthesis?
Children and adolescents with spondylolysis and mild or moderate spondylolisthesis usually heal in about three to four months with rest, bracing, and physical therapy. Children who have spinal fusion surgery for severe spondylolisthesis typically heal in about six months to a year.
Most children who follow the activity restrictions and physical therapy program prescribed by their doctor can return to regular activity once their spine has healed. If your child is at risk of re-injury, their doctor may recommend that they stop playing certain sports.

